

Abstract
Background
Induction therapy for acute myeloid leukemia (AML) with a cytarabine-anthracycline regimen (7+3) is well-established; however, there is no standard salvage therapy for patients with relapsed/refractory AML (RR-AML). There is a paucity of data regarding outcomes with salvage regimens in RR-AML that include cladribine, cytarabine, and filgrastim with mitoxantrone (CLAG-M) or without mitoxantrone (CLAG), and mitoxantrone, etoposide, and cytarabine (MEC). We compared outcomes of patients receiving CLAG-M, CLAG or MEC as salvage therapy for RR-AML.
Methods
A multi-center retrospective study was conducted, including 146 adult RR-AML patients who underwent salvage therapy at the University of Wisconsin and Medical College of Wisconsin from 2009 to 2018. Demographic, clinical and pathologic factors were ascertained at the time of RR-AML diagnosis. The Center for International Blood and Marrow Transplant Research (CIBMTR) response criteria were used. Refractory AML was defined as failure to achieve remission after one or more courses of induction chemotherapy. Minimal residual disease (MRD)-negative was defined by the absence of leukemic cells by morphology and flow cytometry (<0.01%). Data were analyzed using SPSS version 21 (SPSS Inc, Chicago, IL). Bivariate analyses, using chi-square and t-test, and logistic regression analyses were performed for baseline characteristics and response to salvage chemotherapy. Kaplan-Meier analyses, using the log-rank test, were conducted. Cox regression analyses were used to correlate factors with OS. Hazard ratios (HR) with 95% CI were obtained. Statistical significance was considered at P<0.05.
Results
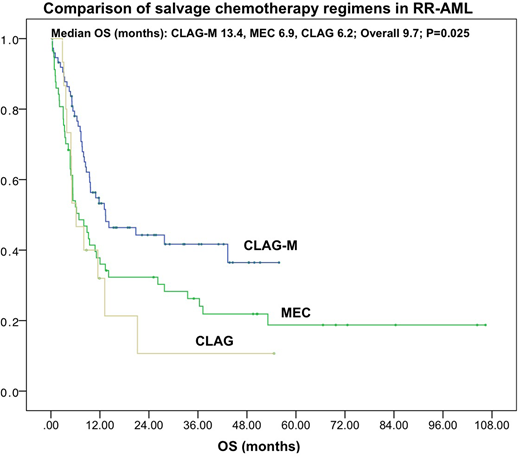
The study included 146 patients with relapsed (57.5%, n=84) or refractory (42.5%, n=62) AML who received CLAG-M (51%, n=74), MEC (39%, n=57) or CLAG (10%, n=15) salvage chemotherapy. Baseline characteristics were similar between the three groups (all P>0.1). Median age was 60 years (range 22-77 years) and 59% patients were male. AML was classified according to WHO 2016 guidelines as AML with recurrent genetic abnormalities (23%), myelodysplasia (MDS)-related AML (25%), therapy-related AML (8%) and AML not otherwise specified (44%). Cytogenetics were good (5%), intermediate (60%) and poor (36%) with normal (41%), complex (25%), trisomy (8%) and monosomy 5 or 7 (5.5%) being common karyotypes. Among those who had molecular testing (n=119), NPM1 and FLT3-ITD were reported in 21% and 20% patients respectively. AML risk status was good (16%), intermediate (32%) and poor (52%), based on cytogenetic and molecular abnormalities as per ELN 2017 and NCCN 2018 guidelines. Extramedullary disease was present in 13% patients. Prior hematopoietic stem cell transplant (HSCT) was performed in 13% patients. Median lab values prior to salvage regimen were: hemoglobin 9.1 g/dL, platelets 49 K/uL, leukocytes 2.5 K/uL, LDH 231 U/L and bone marrow myeloblasts 28%. Overall response rate was 49% (CLAG-M 55%, n=41/74; MEC 44%, n=25/57, CLAG 40%, n=6/15) with complete remission (CR) rate of 46% (CLAG-M 54%, MEC 37%, CLAG 40%) [P=0.140]. Three percent patients (n=5; CLAG-M=1, MEC=4) had CR with incomplete hematologic recovery (CRi). MRD analysis was available for 83 patients and a trend was seen in MRD-negative CR rates favoring CLAG-M (44%) over MEC (25%) or CLAG (17%) [P=0.128]. Sixty-six patients (45%) received subsequent HSCT (CLAG-M 50%, n=37/74; MEC 44%, 25/57; CLAG 27%, n=4/15) [P=0.245]. At last follow-up, 34% patients were in CR (CLAG-M 42%, MEC 28%, CLAG 20%) [P=0.120]. Fifty (34%) patients were alive at last follow-up (CLAG-M 46%, MEC 23%, CLAG 20%) [P=0.010]. Median OS was 9.7 months (95% CI 6.8-12.6) that was significantly better with CLAG-M (13.3 months, 95% CI 2.4-24.3) compared to MEC (6.9 months, 95% CI 2.9-10.9) or CLAG (6.2 months, 95% CI 2.4-12.6) [P=0.025] Figure 1. In multivariate model adjusted for age, gender and refractory vs relapsed AML, MEC (HR 1.75, 95% CI 1.13-2.71, P=0.013) and CLAG (HR 1.97, 95% CI 1.02-3.79, P=0.043) regimens had worse OS compared to CLAG-M. After adjusting for age, gender, refractory vs relapsed AML and HSCT, CLAG-M remained independent predictor of better OS (HR 0.64, 95% CI 0.42-0.97, P=0.037).
Conclusion
CLAG-M compared to MEC or CLAG is associated with significantly better OS in RR-AML regardless of age, refractory vs relapsed AML and HSCT. Our findings support the use of CLAG-M as a preferred salvage regimen for RR-AML.
Atallah:Novartis: Consultancy; BMS: Consultancy; Jazz: Consultancy; Abbvie: Consultancy; Pfizer: Consultancy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal